CRS
- CRS occurred in 51% (80/157) of patients with large B-cell lymphoma (LBCL) receiving EPKINLY at the recommended dosage schedule in EPCORE NHL-1 (37% Grade 1, 17% Grade 2, and 2.5% Grade 3) and recurred in 31% of patients. Most events (92%) occurred during Cycle 1. In Cycle 1, CRS events occurred in 6% of patients after the 0.16 mg dose (Cycle 1, day 1), 12% after the 0.8 mg dose (Cycle 1, day 8), 43% after the first 48 mg dose (Cycle 1, day 15), and 5% after the next 48 mg dose (Cycle 1, day 22). The median time to onset of CRS from the most recent administered dose across all doses was 24 hours (range: 0-10 days). The median time to onset after the first full 48 mg dose was 21 hours (range: 0-7 days).
- CRS occurred in 49% (42/86) of patients with FL receiving EPKINLY monotherapy at the recommended dosage schedule in EPCORE NHL-1 (45% Grade 1, 9% Grade 2) and recurred in 48% of patients. Most events (88%) occurred during Cycle 1. In Cycle 1, CRS events occurred in 12% of patients after the 0.16 mg dose (Cycle 1, day 1), 6% after the 0.8 mg dose (Cycle 1, day 8), 15% after the 3 mg dose (Cycle 1, day 15), and 37% after the first 48 mg dose (Cycle 1, day 22). The median time to onset of CRS from the most recent administered dose across all doses was 59 hours (range: 0.1-7 days). The median time to onset after the first full 48 mg dose was 61 hours (range: 0.1-7 days).
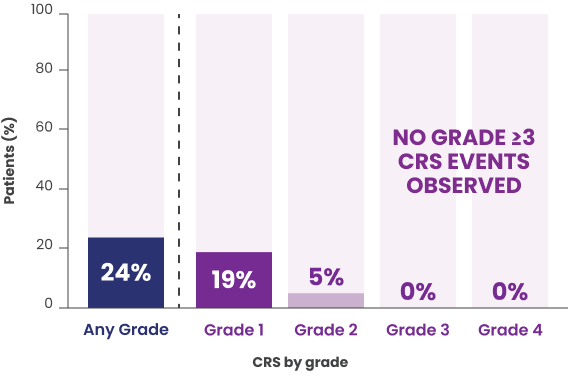
- CRS occurred in 24% (32/131) of patients with FL receiving EPKINLY at the recommended dosage schedule in combination with lenalidomide and rituximab in EPCORE FL-1 (19% Grade 1, 5% Grade 2, and 12% serious adverse reactions due to CRS) and recurred in 41% of patients. Most events (88%) occurred during Cycle 1. In Cycle 1, CRS occurred in 5% of patients after the 0.16 mg dose (Cycle 1, day 1), 3.8% after the 0.8 mg dose (Cycle 1, day 8), 2.3% after the 3 mg dose (Cycle 1, day 15), and 18% after the first 48 mg dose (Cycle 1, day 22). The median time to onset of CRS from the most recent EPKINLY dose was 78 hours (range: 0.2-12 days). The median time to onset after the first 48 mg dose was 41 hours (range: 0.3-12 days).
- For patients with LBCL and FL, assess whether hospitalization or outpatient monitoring for the first 48 mg dose is appropriate based on comorbidities or other situational factors. During outpatient monitoring after the first 48 mg dose, patients should remain in proximity to a healthcare facility that can assess and manage CRS.
- In patients who experienced CRS, the signs and symptoms included pyrexia, hypotension, hypoxia, dyspnea, chills, and tachycardia. CRS resolved in 98% of patients; the median duration of CRS events was 2 days (range: <1-27 days). Concurrent neurological adverse reactions associated with CRS occurred in 2.5% of patients with LBCL, 4.7% of patients with FL receiving EPKINLY monotherapy, and 1.5% of patients receiving EPKINLY in combination with lenalidomide and rituximab (reactions included headache, confusional state, tremors, dizziness, and ataxia).
- Administer pretreatment medications to reduce the risk of CRS.
- Monitor patients for potential CRS. At the first signs or symptoms of CRS, immediately evaluate patients for hospitalization, manage per current practice guidelines, and administer supportive care as appropriate.
ICANS
- ICANS occurred in 6% (10/157) of patients with LBCL receiving EPKINLY at the recommended dosage schedule in EPCORE NHL-1 (4.5% Grade 1, 1.3% Grade 2, 0.6% fatal). Of the 10 ICANS events, 9 occurred within Cycle 1 of treatment, with a median time to onset of 16.5 days (range: 8-141 days) from the start of treatment. Relative to the most recent administered dose, the median time to onset was 3 days (range: 1-13 days). The median duration of ICANS was 4 days (range: 0-8 days), with ICANS resolving in 90% of patients with supportive care.
- ICANS occurred in 6% (8/127) of patients with FL receiving EPKINLY monotherapy following the 2-step up dosage schedule in EPCORE NHL-1 (3.9% Grade 1, 2.4% Grade 2). The median time to onset was 22 days (range: 14-66 days) from the start of treatment. Relative to the most recent administered dose, the median time to onset of ICANS was 3 days (range: 0.4-7 days). The median duration of ICANS was 2 days (range: 1-7 days), with ICANS resolving in 100% of patients.
- Among patients with FL who received EPKINLY at the recommended dosage schedule in combination with lenalidomide and rituximab in EPCORE FL-1, ICANS occurred in 0.8% (1/131, Grade 1).
- The onset of ICANS can be concurrent with CRS, following resolution of CRS, or in the absence of CRS. Clinical manifestations of ICANS included, but were not limited to, confusional state, lethargy, tremor, dysgraphia, aphasia, and non-convulsive status epilepticus.
- Monitor patients for potential ICANS. At the first signs or symptoms of ICANS, immediately evaluate patient, provide supportive therapy based on severity, and manage per current practice guidelines.
Infections
- EPKINLY can cause fatal and serious infections. Serious infections, including opportunistic infections, were reported in 15% of patients with LBCL in EPCORE NHL-1 (most common: 4.5% sepsis, 3.2% pneumonia). Fatal infections occurred in 1.3% of patients (1.3% COVID-19).
- Serious infections, including opportunistic infections, were reported in 40% of patients with FL receiving EPKINLY monotherapy, following the 2-step up dosage schedule in EPCORE NHL-1 (most common: 20% COVID-19, 13% pneumonia, 3% urinary tract infections). Fatal infections occurred in 6% of patients (5% COVID-19, 0.8% pneumonia, 0.8% sepsis).
- Among 243 patients with FL who received EPKINLY in combination with lenalidomide and rituximab in EPCORE FL-1, serious infections occurred in 28% of patients. The most common serious infections were pneumonia (15%), COVID-19 (7%), opportunistic infections (5%) and upper respiratory infections (3.3%). The most common opportunistic infections of any grade were cytomegalovirus (CMV) infection (7%) and herpesvirus infection (7%).
- Progressive multifocal leukoencephalopathy (PML), including fatal cases, has occurred in patients treated with EPKINLY. Across a broader clinical trial population, PML was reported in 0.4% (11/3,072) of patients, including in the first-line treatment setting. Of the 11 cases of PML, 6 resulted in fatal outcomes and 1 was unresolved at the time of death.
- Monitor patients for signs and symptoms of infection and treat appropriately. Avoid administration in patients with active infections. Withhold or consider permanent discontinuation of EPKINLY based on severity. Provide Pneumocystis jirovecii pneumonia (PJP) prophylaxis during treatment with EPKINLY and consider prophylaxis against herpesvirus.
Cytopenias
- EPKINLY can cause serious or severe cytopenias. In the clinical trial of patients with LBCL, Grade 3 or 4 decreased neutrophils occurred in 32% (Grade 4, 14%), decreased hemoglobin in 12% (Grade 4, 0%), and decreased platelets in 12% (Grade 4, 7%) of patients. Febrile neutropenia occurred in 2.5% (Grade 4, 0.6%).
- In the clinical trial of patients with FL who received EPKINLY monotherapy following the 2-step up dosage schedule, Grade 3 or 4 decreased neutrophils occurred in 30% (Grade 4, 17%), decreased hemoglobin in 10% (Grade 4, 0%), and decreased platelets in 8% (Grade 4, 4%) of patients. Febrile neutropenia occurred in 3.1% (Grade 4, 0%).
- In patients with FL who received EPKINLY in combination with lenalidomide and rituximab, Grade 3 or 4 decreased neutrophils occurred in 67% (Grade 4, 41%), decreased lymphocytes in 62% (Grade 4, 13%), decreased hemoglobin in 7%, and decreased platelets in 10% (Grade 4, 4.1%) of patients. Febrile neutropenia occurred in 6% (Grade 4, 2.1%).
- Monitor complete blood counts throughout treatment. Based on severity of cytopenias, temporarily withhold or permanently discontinue EPKINLY. Consider prophylactic granulocyte colony-stimulating factor administration as applicable.
Embryo-Fetal Toxicity
- EPKINLY may cause fetal harm when administered to a pregnant woman. Advise females of reproductive potential to use effective contraception during treatment with EPKINLY and for 4 months after the last dose. Verify pregnancy status in females of reproductive potential prior to initiating EPKINLY.
Adverse Reactions
- EPKINLY as monotherapy for LBCL or FL: Most common (≥20%) adverse reactions were CRS, injection site reactions, fatigue, musculoskeletal pain, fever, diarrhea, COVID-19, rash, and abdominal pain. Most common Grade 3 to 4 laboratory abnormalities (≥10%) were decreased lymphocytes, decreased neutrophils, decreased hemoglobin, and decreased platelets.
- EPKINLY in combination with lenalidomide and rituximab for FL: Most common (≥20%) adverse reactions were rash, upper respiratory tract infections, fatigue, injection site reactions, constipation, diarrhea, CRS, pneumonia, COVID-19, and fever. The most common Grade 3 to 4 laboratory abnormalities (≥10%) were decreased neutrophils, decreased lymphocytes, and decreased platelets.
Use in Specific Populations
- Lactation: Advise women not to breastfeed during treatment and for 4 months after the last dose of EPKINLY.
- Geriatric Use: In patients with relapsed or refractory FL who received EPKINLY in EPCORE NHL-1, 52% were ≥65 years old, and 13% were ≥75 years old. A higher rate of fatal adverse reactions, primarily infections, including COVID-19, was observed in patients ≥65 years old compared to younger adult patients. No overall difference in efficacy was observed.
INDICATIONS
DLBCL and High-grade B-cell Lymphoma
- EPKINLY is indicated for the treatment of adults with relapsed or refractory diffuse large B-cell lymphoma (DLBCL), not otherwise specified (NOS), including DLBCL arising from indolent lymphoma, and high-grade B-cell lymphoma (HGBCL) after 2 or more lines of systemic therapy.
This indication is approved under accelerated approval based on response rate and durability of response. Continued approval for this indication may be contingent upon verification and description of clinical benefit in confirmatory trial(s).
Follicular Lymphoma
- EPKINLY is indicated in combination with lenalidomide and rituximab for the treatment of adults with relapsed or refractory follicular lymphoma (FL).
- EPKINLY is indicated as monotherapy for the treatment of adults with relapsed or refractory FL after 2 or more lines of systemic therapy.
Please see full Prescribing Information, including Boxed Warnings.
04/2026 COM-US-EPK-0002601