3L+ FL Treatment Landscape
Despite an increase in the number of available treatments for FL,
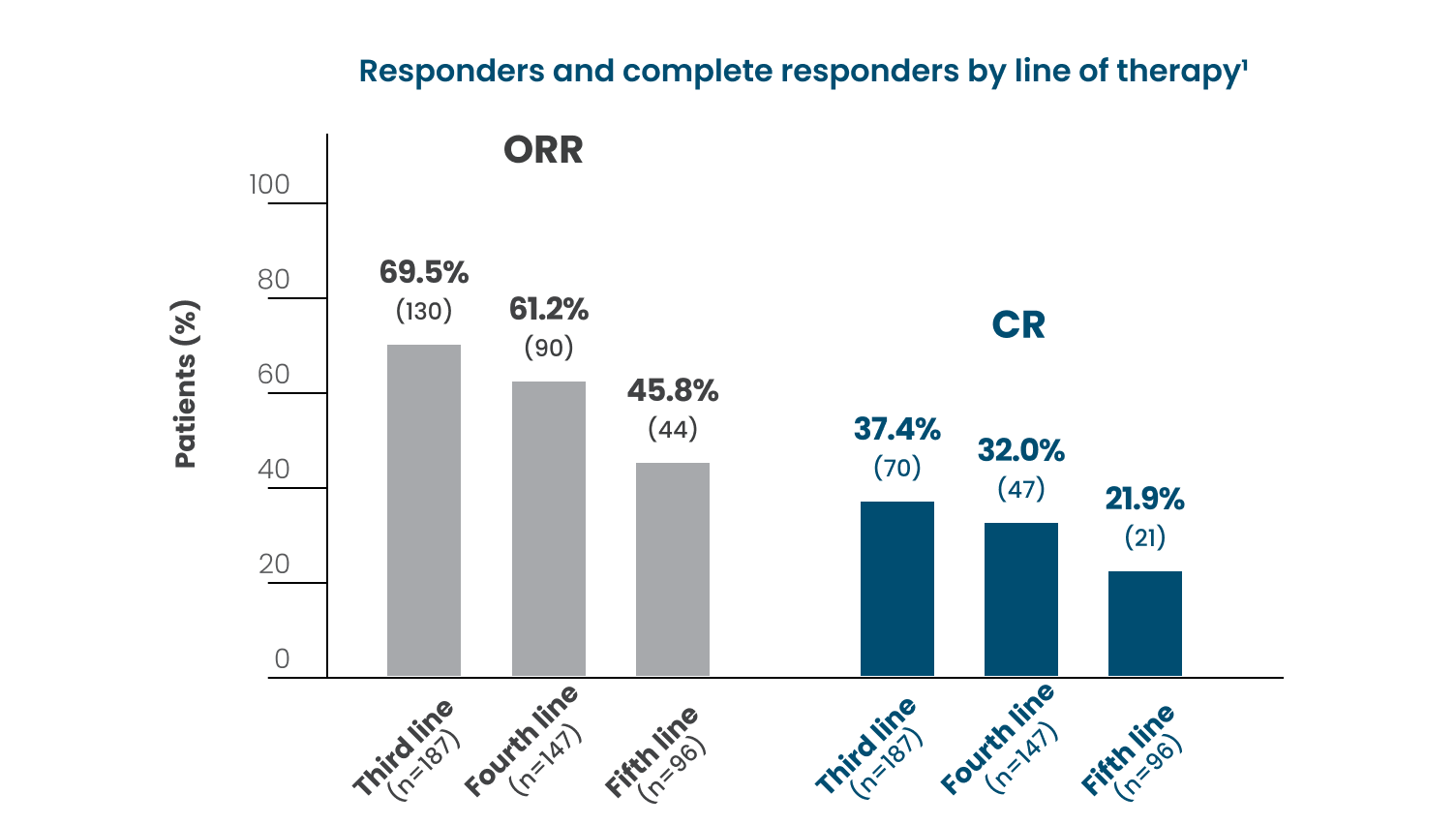
Responses, especially CR, are more difficult to achieve with each subsequent line of therapy1*
Standard front-line therapy options for FL include an anti-CD20 mAb as monotherapy or in combination with chemotherapy. Despite good effectiveness of standard front-line immunochemotherapy treatment, many patients relapse repeatedly with progressively increasing resistance to therapy.1,2
- In a separate retrospective cohort of patients diagnosed with FL, shorter duration between subsequent lines of therapy was observed, indicating faster time to treatment failure3†
CR is increasingly recognized as a clinically meaningful endpoint4:
- CR is used as a primary or secondary endpoint in R/R FL clinical trials
- In a review of a database of 162 trials representing nearly 18,000 patients with FL, MCL, or DLBCL, a correlation was shown between CR and median PFS
*Based on a retrospective cohort study: Medical record review in 10 oncology centers across North America and Europe. Adults with grade 1-3A FL were required to be R/R after ≥2 therapy lines including an anti-CD20 mAb and an alkylator. After first becoming R/R, patients were required to initiate an additional therapy line, which defined the study index date. A total of 187 patients were included in the study.1
†Based on a retrospective observational analysis of US healthcare claims data of 4,232 patients between October 1, 2015 and September 30, 2016. Use of second- and third-line therapies were uncommon, likely due to the short follow-up period. Of the patients who received first-line treatment (n=2,111), 476 received second-line treatment over an average of 2.71 years (SD: 2.1), and 175 received third-line treatment over 2.30 years.3
Certain patient characteristics are linked to worse outcomes5
After 5 years from diagnosis, the risk of lymphoma-related death in patients with FL is5‡:
- 3 times higher for patients aged >70 years vs those aged ≤60 years
- 10 times higher for patients with a high FLIPI score (3 to 5) vs a low FLIPI score (0 to 1)
In a study of FL patients aged ≥66 at diagnosis,6§
- Median OS among 3L patients (n=410) was substantially lower among those classified as double refractory‖ vs those who were not (14.6 months [95% CI, 9.1, 25.4] vs 56.6 months [95% CI, 48.0, 70.1], P<0.0001)
Risk of FL transformation to DLBCL varies; in one study, the rate of transformation was 16% at 10 years7-9¶
- Patients who fail to achieve CR and require ≥2 lines of therapy to control symptomatic FL may be at higher risk of transformation10
In a study of 317 adult patients11#:
- POD24 was associated with an increased risk of aggressive transformation
- The majority of lymphoma-related deaths and all the deaths from transformation occurred in patients with POD24
There is a continued need for tolerable 3L+ FL treatment options that provide durable responses
‡Based on a pooled analysis of 2 independent cohorts in the US and France of a total of 1654 patients with FL. Disease progression, retreatment, transformation, and death events were verified through extensive review of medical records.5
§Based on retrospective, non-interventional, administrative claims database analysis using the Centers for Medicare and Medicaid Service fee-for-service Medicare data.6
‖Patients were classified as double refractory if they initiated new lines of therapy within 6 months after treatment with an anti-CD20 mAb and an alkylating agent.6
¶Risk of transformation based on a retrospective study of 1088 patients with de novo FL diagnosed between 1998 and 2009 and managed at Memorial Sloan Kettering Cancer Center. Patients included in the analysis had FL grade 1-3A and no mixed histology at diagnosis. Transformation was based on biopsy confirmation.9
#Based on an observational, retrospective, monocentric, registry-based study of patients in France aged ≥18 years with FL; investigated POD24 as a predictive value, regardless of the nature of frontline treatment.11
3L=third line; CD20=cluster of differentiation 20; CI=confidence interval; CR=complete response; DLBCL=diffuse large B-cell lymphoma; FL=follicular lymphoma; FLIPI=Follicular Lymphoma International Prognostic Index; mAb=monoclonal antibody; MCL=mantle cell lymphoma; ORR=overall response rate; OS=overall survival; PFS=progression-free survival; POD24=progression of disease within 24 months; R/R=relapsed or refractory; SD=standard deviation.
Learn more about a treatment option for 3L+ FL